

Background: Primary HLH is a rare, life-threatening immune disorder characterized by a hyperinflammatory state. In patients with primary HLH, interferon gamma (IFNy) is often markedly elevated and is considered one of the key cytokine driving the hyperinflammatory state. The treatment goal of primary HLH is to stabilize the disease by controlling the associated hyperinflammation to bring patients to allogeneic hematopoietic stem cell transplantation, the only curative therapy. Conventional HLH therapy comprises immunotherapies (namely, dexamethasone and etoposide), which, unfortunately, predispose patients to infections and toxicity. Emapalumab is a fully human, anti-IFNy monoclonal antibody that neutralizes IFNy. Currently, there is no regulatory precedent or validated response criteria for efficacy assessment to guide clinical trials in primary HLH. In the pivotal study of emapalumab in primary HLH, objective response criteria were used to define the primary endpoint of overall response (Locatelli et al NEJM 2020). These response criteria were defined based on the Histiocyte Society HLH diagnostic criteria (Henter et al Pediatr Blood Cancer 2007), clinical considerations from the study's Scientific Steering Committee, and available experience reported with conventional HLH treatments. We now report on findings of a sensitivity analysis of overall response rate (ORR) to emapalumab using various assessment criteria.
Methods: The open-label pivotal study included patients aged ≤18 years with a diagnosis of primary HLH and active disease (NCT01818492; Locatelli et al NEJM 2020). The initial dose of emapalumab was 1 mg/kg given intravenously every 3 days. Subsequent doses could be increased to 10 mg/kg if required, based on predefined laboratory and clinical response parameters, for a treatment duration of 8 weeks. In addition to emapalumab, all patients received dexamethasone, and a protocol amendment allowed for concomitant use of other HLH treatments if deemed appropriate by the investigator. ORR at end of treatment was analyzed as per the protocol definition in the 27 patients previously treated with conventional therapies. In addition, several pre-specified and post hoc sensitivity analyses were performed to pressure test the data; including: (i) a pre-specified analysis using a more conservative approach where any patient who received concomitant HLH therapies during the study was imputed as non-responder; (ii) a pre-specified analysis with physician-reported response rates recorded by the study investigators, based on their clinical judgement and previous experience in treating patients with primary HLH; and (iii) a post hoc sensitivity analysis using a previously published definition of overall response (Henter et al Pediatr Blood Cancer 2007).
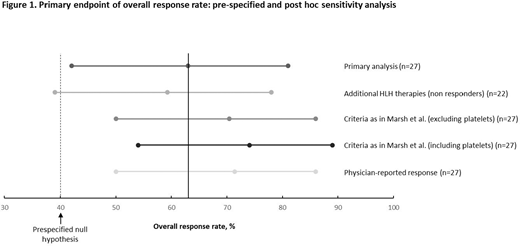
Results: 63% (95% confidence interval [CI], 0.42, 0.81) of 27 treatment-experienced patients had a response according to the pivotal study protocol definition of ORR (Fig. 1). A pre-specified sensitivity analysis on the primary endpoint where any patient who received concomitant HLH therapy and imputed as non-responders showed a magnitude of response similar to that observed in the protocol-defined primary analysis (59.3%; 95% CI 0.39, 0.78; n=22). Use of the response criteria defined by Marsh et al (Pediatr Blood Cancer 2013) in a retrospective analysis of 27 patients with primary HLH also resulted in a similar ORR to the protocol-defined primary endpoint in treatment-experienced patients (70.4%; 95% CI 0.50, 0.86). When platelet count was added to this analysis, the percentage of responders to emapalumab increased to 74.1% (95% CI 0.54, 0.89). The pre-specified analysis of physician-reported response rates was also in line with the primary analysis, with 70.4% (95% CI 0.50, 0.86) of 27 treatment-experienced patients deemed to have a response to emapalumab.
Conclusion: The current analyses using different definitions of treatment response support the primary analysis results by having a numerically comparable point estimate to the primary endpoint, therefore confirming the positive benefit of emapalumab in patient's refractory or intolerant to conventional HLH therapies. Taken together, these findings also suggest that the clinically objective ORR, utilized in the pivotal emapalumab trial, may be used as a primary endpoint in primary HLH.
Locatelli:Jazz Pharmaceeutical: Speakers Bureau; Medac: Speakers Bureau; Miltenyi: Speakers Bureau; Bellicum Pharmaceutical: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Jordan:Sobi: Consultancy. Allen:Sobi: Other: Scientific Steering Committee, Data And Safety Monitoring. Rizzari:Sobi: Consultancy, Other: Advisory Board. Rao:Sobi: Consultancy, Other: Advisory Board. Sevilla:Amgen: Other: Advisory Board; Rocket Pharma: Consultancy; Sobi: Other: Advisory Board; Novartis: Other: Advisory Board. Henry:Sobi: Consultancy. De Benedetti:Abbvie: Research Funding; F Hoffmann-La Roche AG: Research Funding; Novartis Pharma: Research Funding; Pfizer: Research Funding; Sanofi-Aventis: Research Funding; Sobi: Consultancy, Research Funding. Grom:Sobi: Consultancy; Novartis Pharma: Consultancy; AB2Bio: Consultancy. Stoltenberg:Sobi: Current Employment. Vågerö:Sobi: Consultancy. de Min:Sobi: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal